Around 35 million people are hospitalized annually, with each patient requiring medical charts that contain data that could improve outcomes if it were actually accessible.
The reality of clinical data abstraction is often less about high-level insights and more about a frantic race against registry deadlines. Most teams treat abstraction as a manual chore rather than a structured pipeline, which leads to backlogs that never seem to shrink.
An Overview of Data Abstraction
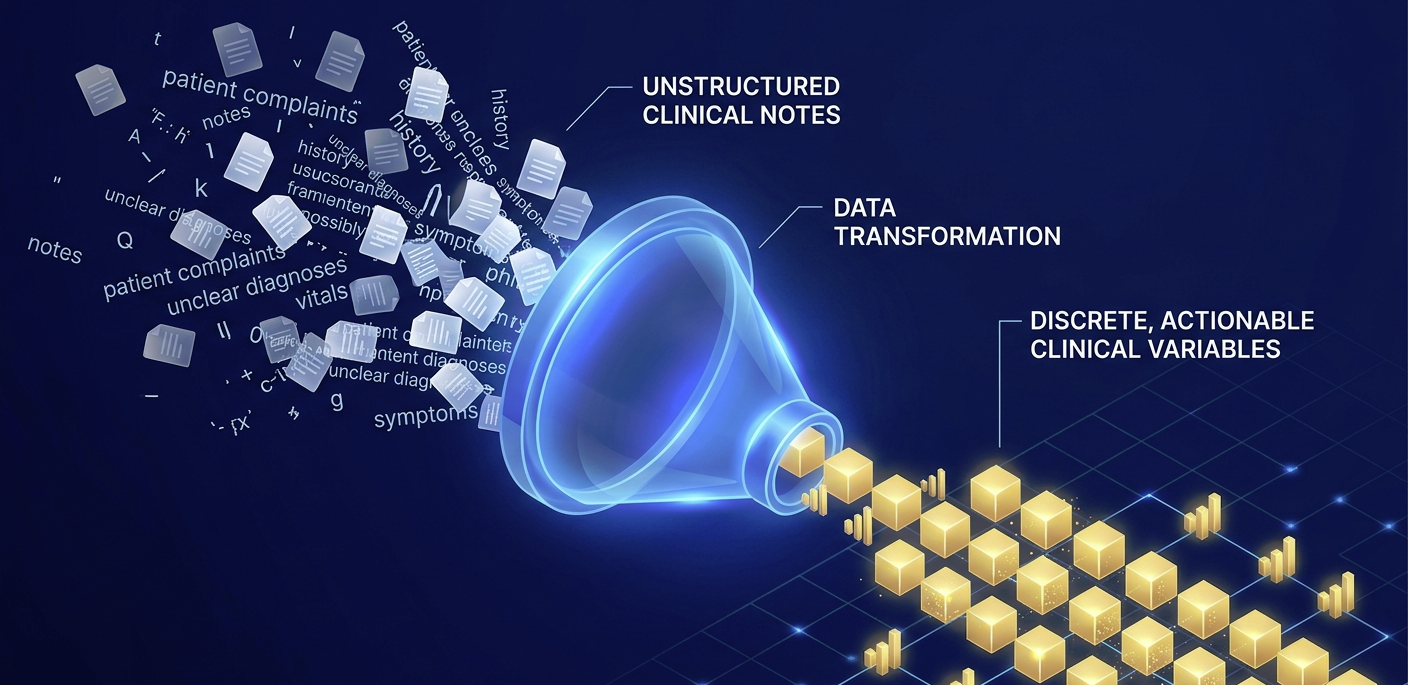
Clinical data abstraction transforms raw, unstructured narrative notes into the discrete variables required by national registries and quality reporting programs. When this process stalls, the hospital loses the ability to track performance in real time.
Moving toward a streamlined model requires more than just hiring more staff. It involves a fundamental shift in how data moves from the clinician’s keyboard to the final report.
Standardization starts with a definitive source-of-truth map. Many abstractors waste hours debating whether a specific lab value from a specialist’s note overrides a different value in the discharge summary.
Establishing a hierarchy of documentation prevents these micro-decisions from compounding into significant delays. Once the mapping is clear, the workflow can finally move at a predictable pace.
The complexity of modern reporting often makes outsourcing data abstraction a logical choice for facilities facing fluctuating patient volumes. Professional partners often bring existing frameworks for measure specification mapping that internal teams might still be building from scratch. This allows internal quality leaders to focus on the “so what” of the data rather than the “how” of the collection.
Building A Repeatable Abstraction Workflow
Efficiency is not a happy accident. It is the result of a deliberate sequence that removes friction from the abstractor’s daily routine, just as the right platform can optimize operations in a business context. The most successful quality departments utilize a tiered approach to ensure that high-level clinicians are not spending their time on basic data entry.
Standardizing templates is the first step toward a faster turnaround. If every abstractor looks for smoking status or ejection fraction in a different part of the EHR, the process will always be slow. Creating a unified digital workspace where the required fields match the flow of the clinical record is essential for speed.
A streamlined workflow generally includes these three primary pillars:
- Consistent mapping of measure specifications to specific EHR fields
- Real-time access to clinical documentation through integrated viewer tools
- Regular inter-rater reliability testing to ensure data consistency
Once these pillars are in place, the focus shifts to quality gates. You cannot wait until the end of a reporting quarter to check for errors. Implementing weekly QA checks allows for immediate course correction. This prevents a small misunderstanding of a new registry definition from turning into a thousand-record mistake that requires a total rewrite.
The Role Of Technology And Human Oversight
We are entering an era in which Natural Language Processing (NLP) can do the heavy lifting of finding specific phrases across thousands of pages of text. Recent studies show that Large Language Models can achieve 90% accuracy in identifying core clinical variables. This does not replace the human element, but it changes the job description from “hunter-gatherer” to “editor-verifier.”
Technology should act as a nudge. It flags the relevant section of the chart, highlights the potential data point, and lets the professional abstractor make the final call. This “human-in-the-loop” model enables a 40% reduction in turnaround time without compromising the integrity of the registry.
Maintaining high Inter-Rater Reliability (IRR) is the only way to ensure that the data being reported to the Joint Commission or CMS is actually representative of the care provided. If two different abstractors look at the same chart and reach different conclusions, the data is noise. Regular IRR sessions where the team reviews “gray area” charts together will naturally sharpen the collective accuracy of the group.

Managing Staffing Models For Predictable Results
Burnout is a significant risk in the abstraction world. The work is repetitive, the deadlines are rigid, and the stakes for accuracy are incredibly high. Simple dashboards that track “charts per hour” can be helpful, but they can also be demoralizing if they don’t account for the complexity of the cases being reviewed.
A better approach is to use a weighted productivity model. A simple outpatient encounter should not “count” the same as a complex cardiac surgery case with forty different variables.
By weighting the workload, management can create a staffing model that is actually predictable. This allows for better planning during seasonal surges in patient volume or when new registry requirements are introduced.
Audit preparation should be a year-round activity rather than a seasonal panic. When the workflow is standardized, the “paper trail” for every data point is created automatically. This means that when an auditor asks why a certain patient was excluded from a cohort, the abstractor can point directly to the logic used during the initial review.
Evolving Your Quality Reporting Strategy
The transition from manual labor to a streamlined, tech-assisted pipeline is no longer optional for high-performing hospitals. As the volume of clinical data continues to explode, the old methods of “find and enter” will inevitably break under the pressure.
The goal is to create a system that is resilient enough to handle new measures without requiring a total overhaul of the department.
By focusing on source-of-truth definitions and robust QA gates, healthcare organizations can turn their data abstraction from a bottleneck into a competitive advantage. Accurate data leads to better clinical decisions, which ultimately leads to better patient care. The work of the abstractor is the foundation upon which the entire quality improvement structure is built.
For more information on improving the operational aspects of many organizations, not just in healthcare, read our other posts and see where they take you.